Overview
Anatomical Target and Coverage
This peripheral nerve block targets the cords of the brachial plexus1. It provides anesthesia and analgesia to the upper arm, elbow, forearm and hand. It does not block the intercostal brachial nerve (T2). However, it rarely requires supplementation for the use of an arm tourniquet.
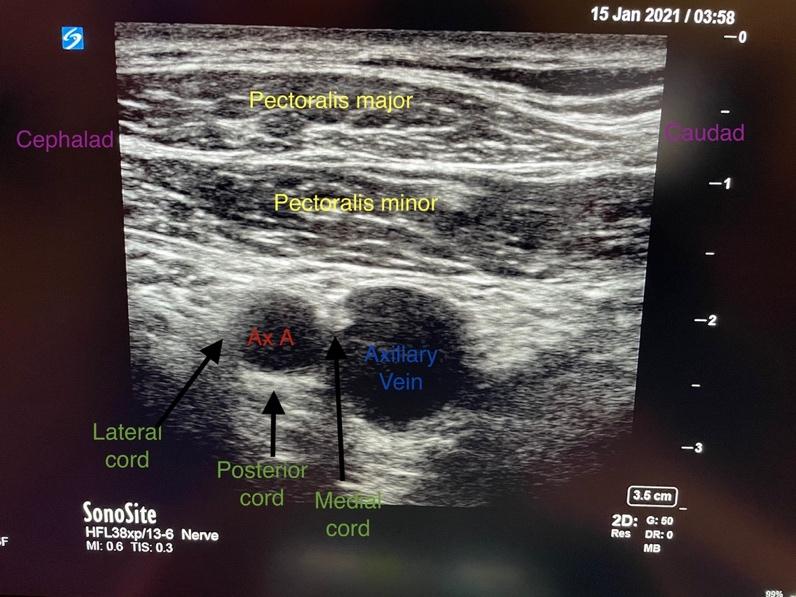
The divisions of the brachial plexus and subclavian artery pass between the clavicle and first rib, entering the infraclavicular fossa. The cords are found deep to the pectoralis major and minor muscles. The cords are referred to as the lateral, posterior and medial based on their association to the axillary artery.
Indications
Provision of analgesia and anesthesia for procedures below the mid-humerus, elbow, forearm, wrist, and hand.
Block Technique
The block is performed with ultrasound in a supine patient using an in-plane approach from cephalad to caudad. The arm is often placed at the patient's side or abducted (reducing the depth to the cords of the plexus). The ultrasound is placed beneath the clavicle over the lateral chest wall (see image below). A single-shot injection or catheter can be placed, with the benefit of comfort and location when using a continuous peripheral nerve infusion.

Dosing
Adult patients >60kg
Single shot: 20-30ml of 0.5% ropivacaine
Infusion: 8ml/hour 0.1-0.2% ropivacaine
Block Duration
When performed with ropivacaine, the infraclavicular block has an analgesia duration of hours 6-10 hours.2
When longer block duration is required, a catheter-based technique can be used to allow continuous infusion of the local anesthetic thus providing analgesia for days if needed.
Special Considerations
Contraindications, side effects and complications
Patient refusal, coagulopathy, local anaesthetic allergy, systemic infection in the needle trajectory, chest deformities, dislocation or fracture of the clavicle, infection, hematoma, pneumothorax (0.7%), phrenic nerve palsy (3%), nerve damage and systemic absorption of local anesthetic.
Phrenic nerve palsy may occur if a large volume of local anesthesia is used and therefore if the patient has brittle lung disease, this may be a relative contraindication to the block. The infraclavicular block can provide a more reliable block of the ulnar nerve than more proximal approaches, with fewer episodes of phrenic nerve palsy, pneumothorax, and Horner’s syndrome.
Who do I contact if I feel my patient could benefit from a regional anesthesia technique?
When booking OR cases, surgeons can enter requests for regional anesthesia. The Department of Anesthesia schedules experienced providers to perform these blocks in all ORs. For regional anesthesia in inpatients reach out to the Acute Pain Service that covers your campus.
Please see the link for the pain team consult service:
https://anesthesia.ucsf.edu/divisions/pain-medicine#for-providers--request-consult-or-refer-a-patient
References
- Chin KJ, Alakkad H, Adhikary SD, et al. Infraclavicular brachial plexus block for regional anaesthesia of the lower arm. Cochrane Database Syst Rev. 2013;28(8):CD005487
- Abdallah FW, Halpern SH, Aoyama K, et al. : Will the Real Benefits of Single-Shot Interscalene Block Please Stand Up? A Systematic Review and Meta-Analysis. Anesth Analg. 2015;120(5):1114–29